|
 |
The UKHSA review of influenza H5N1 Incubation and Infectiousness
More poor quality work to throw petrol on the flames
The UKHSA have just produced a “review that aims to identify and summarise evidence relating to the infectious and incubation period of influenza (H5) up to 26 April 2024. “A rapid evidence summary was conducted, following streamlined, systematic methods to accelerate the review process.”
Incubation and infectious period of influenza A (H5). A rapid evidence summary
We reported on this in our post:

The aim of the review was as follows:
 |
Some points stand out in the review’s protocol. For example, the protocol states that the ‘Risk of bias of included studies will not be assessed in this rapid evidence summary due to time constraints.’ With a budget of over £3 billion and eight months to assess the quality we find this explanation ridiculous - It’s not the first time that the UKHSA uses this excuse to cover shoddy work,
Therefore, we thought we’d have a look at the 11 studies included in the review.
We did not repeat the searches but quality assessed the 11 studies Identified by UKHSA.
You can find the details of our extraction here:
| ||
Given the design of the 11 included studies omission of risk of bias is very relevant to the conclusions of the studies and the review.
The other linked point worthy of note is what the authors considered as proof of infectiousness and transmission. We are not clear. Here is how the protocol puts it:
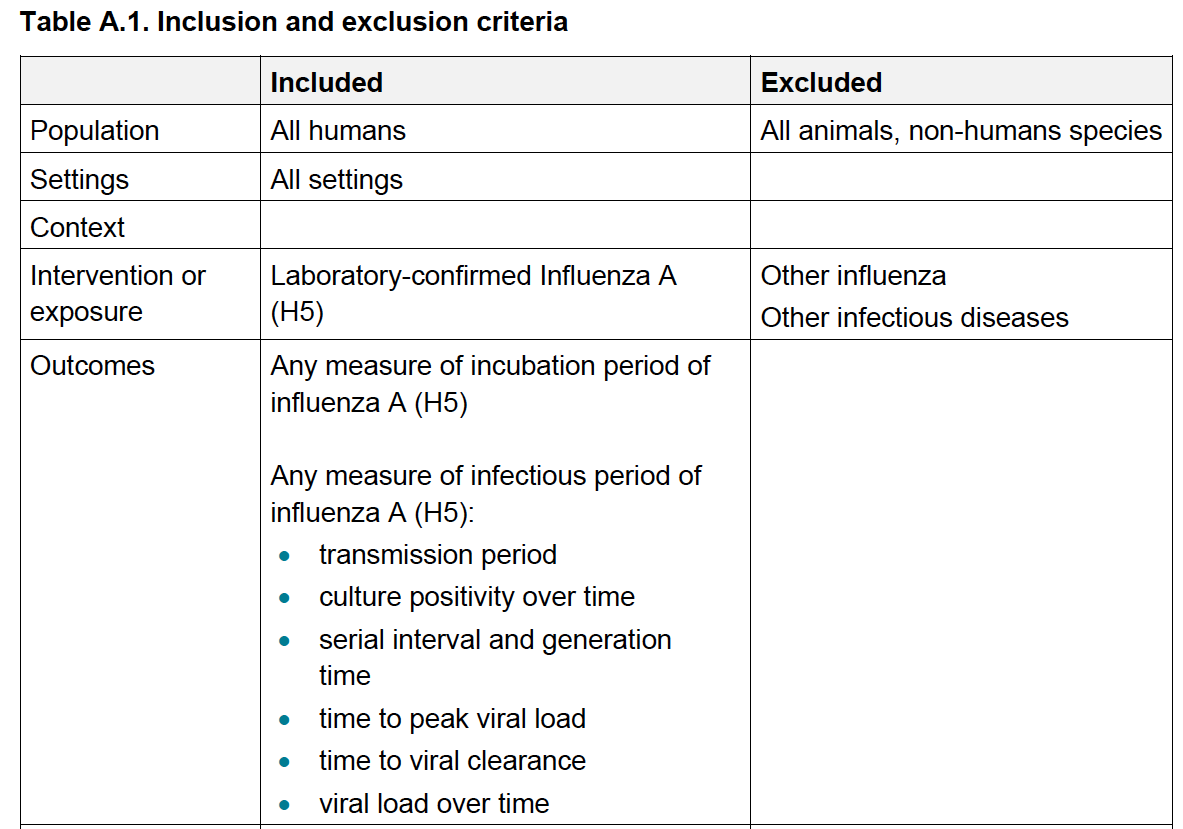 |
The focus is only on the H5N1 subtype - Why drop the N1, by the way? Is there something we don’t know?
An outcome of “any measure” is a bit vague. Viral load is mentioned several times in the outcomes but not at all in the exposure. Let’s be clear. The review is about infectiousness (the potential for A to pass onto B) and the incubation period (when B has no symptoms and goes around kissing people before feeling sick). Transmission cannot occur if you are not exposed to an infectious (i.e., replication-competent) virus in a dose that is likely to cause problems.
And how did the authors quantify the infectious dose or likelihood of infection?
As you will see from the sheet, we assessed six studies as very low quality, two as low quality, and the rest as moderate quality. The main problems with each study are highlighted in bold in Comments column of the sheet.
The main recurring problems are the confirmation of infectiousness and active disease and the generalisability of results from the original settings to better hygiene conditions and less promiscuity with animals. None of the studies measured viral load or reported the PCR cycle threshold. This is a vital piece of the jigsaw to establish whether the individuals were infectious during testing or contaminated through contact with poultry.
In Oner 2006, All the samples were negative for the H5N1 virus on the rapid influenza and ELISA tests. However, the virus was detected in 10 patients using real-time PCR. The discrepancy suggests RT-PCR positives are likely contamination. This issue is further highlighted in a review of 2 case clusters. Wang 2008 reported that they did not isolate any more than one H5N1 virus from either case and were unable to assess viral load in serial clinical specimens because the quality of the specimens was suboptimal.
In Ungchusak 2005, the criteria for establishing the diagnosis in the index could not be verified. By the time this family cluster was recognised, the index patient had died, and her body had been cremated, and the mother had died, and her body had been embalmed; therefore, obtaining appropriate specimens was - putting it mildly - difficult ot obtain. In Huang 2008, it was more than difficult: Laboratory testing was not performed to confirm that the exposure sources contained influenza virus (H5N1) or to quantify exposures.
We also found several studies that the UKHSA searches missed. The UKHSA review does not advance our understanding of transmission, both because of the poor quality of the original studies and the lack of strategic vision in laying down clear rules for grading evidence of transmission.
Despite this being the biggest issue in the global pandemic threat catalogue, there is a reluctance to share data, hampering progress. Yang 2007 reported that virus isolates from six of the eight family members had been sequenced, but the WHO had refused to release the data, saying that they. A Nature editorial about the research notes, “part of the reason the picture is so unclear, say virologists, is that the continued withholding of genetic data is hampering study of the virus”.
Indeed, the picture is unclear. Perhaps transmission should be better studied before sinking a load of taxpayers’ money in an H5 vaccine.
 |
|
This post was written by two old geezers who can confirm that they have not been exposed to live chickens, have not been to a wet chicken market, and do not keep chickens in their gardens or under their beds.
Invite your friends and earn rewards
![]()
![]()